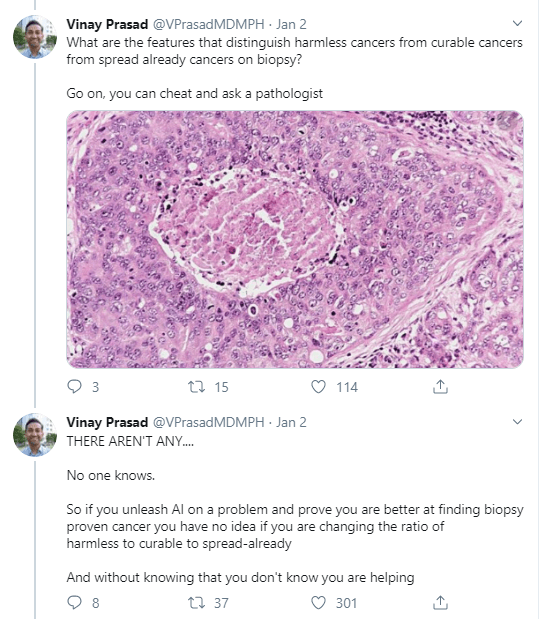
I came across this opinionated though informed commentary by Vinay Prasad on the recent Nature article where Google’s machine learning experts trained models to predict whether scans of patients’ breasts (mammogram’s) show cancerous cells or not.
Vinay Prasad [official bio] is a practicing hematologist-oncologist and Associate Professor of Medicine at Oregon Health and Science University. So he knows what he’s talking about.
He argues that “cancer screening is the LAST thing you should pick FIRST to work on with AI”. Which is an interesting statement in and of itself.
Regardless of my personal opinion on the topic, I found the paper, Vinay’s commentary, and the broader discussion on twitter very interesting and educational to read. I feel it shows how important it is to know the context in which you are applying machine learning. What tremendous value it provides to have domain experts in the same team as the data and machine learning experts.
Frank Harrel shared this 16-page glossary of statistical terminology created by the Department of Biostatistics of Vanderbilt University School of Medicine. The overview touches on everything from Bayes’ Theorem to p-values, explaining matters in just the right detail. Various study designs and model types are also discussed so it might just come in handy for a quick review or just to browse through and see what you might have missed past years.
The below reiterates and summarizes this Stat article.
Recently, I addressed how bias may slip into Machine Learning applications and this weekend I came across another real-life example: IBM’s Watson, specifically Watson for Oncology. With a single machine, IBM intended to tackle humanity’s most vexing diseases and revolutionize medicine and they quickly zeroed in on a high-profile target: cancer.
However, three years later now, a STAT investigation has found that the supercomputer isn’t living up to the lofty expectations IBM created for it. IBM claims that, through Artificial Intelligence, Watson for Oncology can generate new insights and identify “new approaches” to cancer care. However, the STAT investigation (video below) concludes that the system doesn’t create new knowledge and is artificially intelligent only in the most rudimentary sense of the term. Similarly, cancer specialists using the product argue Watson is still in its “toddler stage” when it comes to oncology.
Let’s start with the positive side. For specific treatments, Watson can scan academic literature, immediately providing the “best data” about a treatment — survival rates, for example — thereby relieving doctors of tedious literature searches. Due to this transparency, Watson may level the hierarchy commonly found in hospital settings, by holding (senior) doctors accountable to the data and empowering junior physicians to back up their arguments. Furthermore, Watson’s information may empower patients as they can be offered a comprehensive packet of treatment options, including potential treatment plans along with relevant scientific articles. Patients can do their own research about these treatments, and maybe even disagree with the doctor about the right course of action.
Although study results demonstrate that Watson saves doctors time and can have a high concordance rate with their treatment recommendations, much more research is needed. The studies were all conference abstracts, which haven’t been published in peer-reviewed journals — and all but one was either conducted by a paying customer or included IBM staff on the author list, or both. More importantly, IBM has failed to exposed Watson for Oncology to critical review by outside scientists nor have they conducted clinical trials to assess its effectiveness. It would be very interesting to examine whether Watson’s implementation is actually saving lives or making healthcare more efficient/effective.
IBM Watson HealthSuch validation is especially necessary because several issues are identified. First, the actual capabilities of Watson for Oncology are not well-understood by the public, and even by some of the hospitals that use it. It’s taken nearly six years of painstaking work by data engineers and doctors to train Watson in just seven types of cancer, and keep the system updated with the latest knowledge. Moreover, because of the complexity of the underlying machine learning algorithms, the recommendations Watson puts out are a black box, and Watson can not provide the specific reasons for picking treatment A over treatment B.
Second, the system is essentially Memorial Sloan Kettering in a portable box. IBM celebrates Memorial Sloan Kettering’s role as the only trainer of Watson. After all, who better to educate the system than doctors at one of the world’s most renowned cancer hospitals? However, doctors claim that Memorial Sloan Kettering’s training has caused bias in the system, because the treatment recommendations it puts into Watson don’t always comport with the practices of doctors elsewhere in the world. When users ask Watson for advice, the system also searches published literature — some of which is curated by Memorial Sloan Kettering — to provide relevant studies and background information to support its recommendation. But the recommendation itself is derived from the training provided by the hospital’s doctors, not the outside literature.
Doctors at Memorial Sloan Kettering acknowledged their influence on Watson. “We are not at all hesitant about inserting our bias, because I think our bias is based on the next best thing to prospective randomized trials, which is having a vast amount of experience,” said Dr. Andrew Seidman, one of the hospital’s lead trainers of Watson. “So it’s a very unapologetic bias.”
However, this bias causes serious problems when Watson for Oncology is implemented in other countries/hospitals. The generally affluent population treated at Memorial Sloan Kettering doesn’t reflect the diversity of people around the world. According to Martijn van Oijen, an epidemiologist and associate professor at Academic Medical Center in the Netherlands, Watson has not been implemented in because of country level differences in treatment approaches. Similarly, oncologists at one hospital in Denmark said they have dropped implementation altogether after finding that local doctors agreed with Watson in only about 33 percent of cases. Different problems occurred in South Korea, where researchers reported that the treatment Watson most often recommended for breast cancer patients simply wasn’t covered by their national insurance system.
Kris, the lead trainer at Memorial Sloan Kettering, says nobody wants to hear the problems. “All they want to hear is that Watson is the answer. And it always has the right answer, and you get it right away, and it will be cheaper. But like anything else, it’s kind of human.”




![imaging-video[1].jpg](https://paulvanderlaken.com/wp-content/uploads/2017/09/imaging-video1.jpg)
